Urinary tract
Functions of the kidneys:
- Maintain internal environment- renal excretion, water control (baroreceptors, ADH) and Na control (barorecptors)
- Metabolic products excreted- e.g. urea, uric acid and creatinine
- Foreign chemicals excreted- e.g. drugs, pesticides, food additives.
- Secretory gland- EPO (erythrocyte production), 1,25-dihydroxyvitamin S (Ca absorption) and Renin (BP control)
- Gluconeogenesis- although the main site is the liver, some occurs in the kidneys. Synthesise glucose from amino acids and release into blood.
Glomerular filtration Barrier:
- Barrier consists of fenestrated endothelial cells of the capillaries, glomerular basement membrane and podocytes.
- Podocytes are specialised epithelium cells that hover above the basement membrane and project foot processes towards the membrane.
- The filtration slit diaphragm bridges the gap between podocytes. Important proteins involved in the diaphragm are Nephrin (NEPH1 & NEPH2), Podocin and CD2AP.
- In Congenital Nephrotic Syndrome (CNS), no nephrin is present so massive proteinuria occurs along with hypoalbuminaemia, hyperlipidaemia, abdominal distention and oedema.
- Other relevant pathologies include NPHS1 mutation, Nephrin down regulation or redistribution, and nephrin antibodies.
GLOMERULAR FILTRATION RATE:
- GFR- the volume filtered from the glomeruli into Bowman's capsule per unit of time.
- It is determined by: Net filtration pressure, permeability of the capsular membrane and surface area available for filtration.
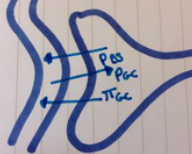
- Favouring fource:glomerular blood pressure (PGC)
- Opposing forces: Fluid pressure in Bowman's space (PBS) . Osmotic force due to protein in plasma (πGC)
- GFR is not fixed: subject to physiological regulation: neural/hormonal, achieved by constriction/dilatation of the efferent and afferent arterioles and input to mesangial cells.
- Mesangial cells have contractile properties and can therefore restrict blood flow and surface area if stimulated- decreasing GFR.
- Filtered load= GFR x plasma concentration of a substance (can be compared to amount excreted and can tell you if the substance undergoes tubular reabsorption or secretion).
Classification of ckdStage 1
Stage 2 Stage 3 Stage 4 Stage 5 |
DetailKidney damage/normal GFR
Mild insufficiency Moderate insufficiency Severe insufficiency Kidney failure |
eGFR>90
89-60 59-30 30-15 <15 |
Sodium reabsorption
This occurs in every tubular segment except the descending limb of the loop of Henle. REMEMBER- water follows sodium! So water diffusion is dependent on sodium reabsorption!
- 60% is reabsorbed in proximal tubule by co-transport.
- 25% in the ascending limb of the Loop of Henle by co-transport.
- 10% in the distal tubule by active transport through Na/Cl channels.
- 4% in the collecting duct.
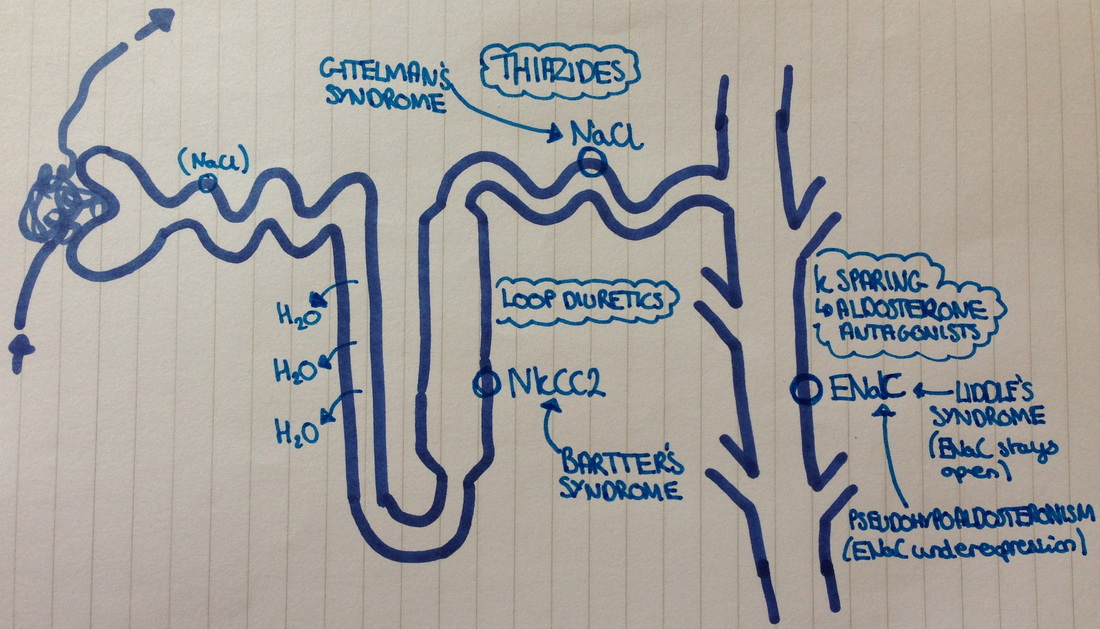
- Bartter's syndrome (type 1- NKCC2, type 2- ROMK, type 3-ClCNKB): has the same effect as loop diuretics.
- hypotension/?normal
- Metabolic alkalosis
- Hypercalcaemia
- Hypokalaemic alkalosis(due to increases RAAS)
- Gitelmann's syndrome: acts on the distal tubule (Nacl/NCCT pump). Same effect as Thiazides.
- Hypotension
- Salt wasting
- Hypocalcaemia
- Hypokalaemic alkalosis (increased RAAS)
- Liddle's syndrome: ENaC stays open in collecting duct. Treat with Amiloride
- Hypertension
- Hypokalaemia
- Hypernutraemia
- Hypokalaemia
- Pseudohypoaldosteronism: ENaC under-expression in collecting duct. Same action as K sparing diuretics (amiloride)
- Hypotension
- Hyperkalaemia
- Increased aldosterone
Sodium and water regulation
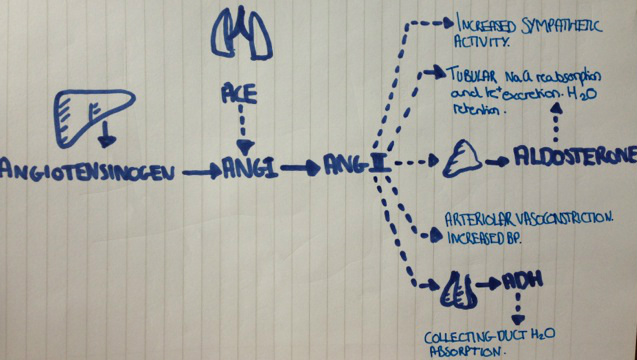
- RAAS system- A drop in blood pressure is detected by baroreceptors (present in the aortic arch and carotid sinus) which then activates the RAAS system- ultimately producing Aldosterone which increases Na reabsorption and therefore acts to increase blood pressure (it also increases K secretion).
- Juxtaglomerular apparatus- Juxta/granular cells (afferent arteriole): secrete renin in response decreased perfusion pressure and when signalled by Macular densa cells (DCT): sense NaCl concentration and regulates feedback. Renin activates the conversion of Angiotensinogen to Angiotensin I.
- This results in increased water and salt retention and an increase in blood pressure. Perfusion of the juxtaglomerular apparatus increases causing negative feedback and homeostasis.
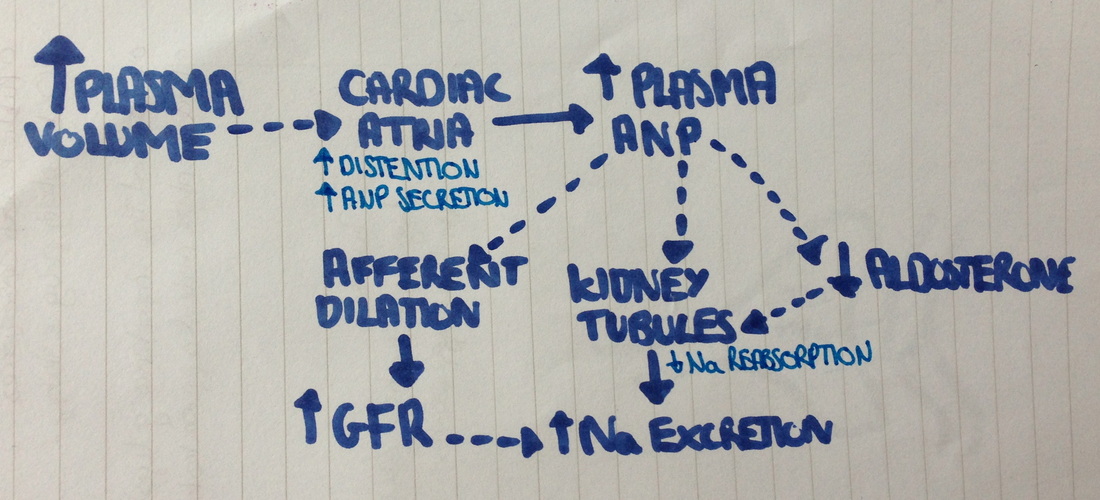
- When plasma volume gets too high, in addition to the negative feedback of the RAAS system, ANP is secreted from the cardiac atria. It has several actions including:
- Vasodilation of the afferent arteriole- increasing GFR
- Inhibits Aldosterone secretion
- Inhibits ADH release
- Decreases renin release
- Acts on the renal tubules, reducing Na reabsorption.
POTASSIUM secretion
My understanding of potassium secretion effects and balance is minimal. But here is a link to some helpful quiz cards: http://quizlet.com/7583718/urinary-system-session-5-potassium-regulation-flash-cards/
