Neuroanatomy
Basics - planes
Sagittal - vertical along sagittal suture
Parasagittal - parallel to sagittal plane
Rostral - Anterior in hemispheres. Superior aspect in spine.
Caudal - Posterior in hemispheres. Inferior aspect in spine.
Ventral - Inferior in hemispheres. Anterior aspect in spine
Dorsal - Superior in hemispheres. Posterior aspect in spine.
Transverse/Axial - 90 degrees to long axis
Coronal - Vertical. 90 degrees to sagittal.
Parasagittal - parallel to sagittal plane
Rostral - Anterior in hemispheres. Superior aspect in spine.
Caudal - Posterior in hemispheres. Inferior aspect in spine.
Ventral - Inferior in hemispheres. Anterior aspect in spine
Dorsal - Superior in hemispheres. Posterior aspect in spine.
Transverse/Axial - 90 degrees to long axis
Coronal - Vertical. 90 degrees to sagittal.
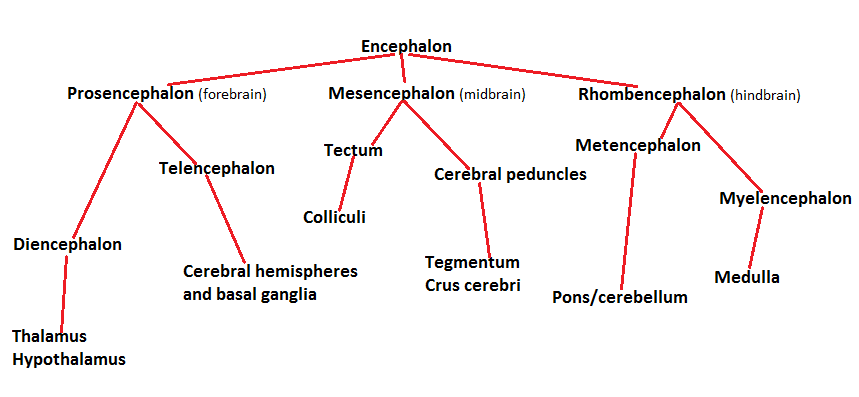
Embryology
Lobes
Frontal - thinking, planning, organising, problem solving, behavioural control, personality
Temporal - memory, understanding language
Parietal - perception, making sense of things, arithmetic, spelling
Occipital - vision
Motor cortex - movement. Primary motor area
Sensory cortex - sensation. Primary sensory area
Broca's area - anterior speech area - language expression. In frontal lobe
Wernicke's area - posterior speech area - language comprehension. In parietal lobe
Temporal - memory, understanding language
Parietal - perception, making sense of things, arithmetic, spelling
Occipital - vision
Motor cortex - movement. Primary motor area
Sensory cortex - sensation. Primary sensory area
Broca's area - anterior speech area - language expression. In frontal lobe
Wernicke's area - posterior speech area - language comprehension. In parietal lobe
Meninges
3 layers...
Dura Mater - made of 2 fused layers. Inner layer separates to form dural folds which the dural venous sinuses sit in
Arachnoid Mater
Pia Mater - forms part of blood brain barrier
spaces between layers
Subdural
Subarachnoid - CSF flows through here. The arteries in the brain lie in the subarachnoid space and with prolongations of pia mater and subarachnoid space to make the blood brain barrier against neurological tissue.
Dura Mater - made of 2 fused layers. Inner layer separates to form dural folds which the dural venous sinuses sit in
Arachnoid Mater
Pia Mater - forms part of blood brain barrier
spaces between layers
Subdural
Subarachnoid - CSF flows through here. The arteries in the brain lie in the subarachnoid space and with prolongations of pia mater and subarachnoid space to make the blood brain barrier against neurological tissue.
Subdural/epidural haematoma
|
Location Involved vessel Symptoms CT appearance |
EpiduralBetween skull and dura
Temperoparietal - middle meningeal artery Frontal - anterior ethmoidal artery Occipital - transverse/sigmoid sinus Vertex - superior sagittal sinus Lucid interval before unconscoiusness Biconvex lens |
subduralBetween dura and arachnoid
Bridging veins Gradually increasing headache and confusion Crescent shaped |
Main cause of subdural haematoma is head injury such as 'shaken baby syndrome'
Main cause of epidural haematoma is trama
Treat by surgically removing blood/clot etc
Main cause of epidural haematoma is trama
Treat by surgically removing blood/clot etc
Dural venous sinuses
Found on the borders of dura mater reflections - Falx cerebri, Tentorium cerebelli.
Eg
The cavernous sinus contains the internal carotid artery. It is the only place in the body where an artery runs through a venous supply. If the artery ruptures then it can cause an arteriovenus fistula.
Also passing through the cavernous sinus is the occulomotor, trochlear, opthalmic and maxillary nerves
Eg
- Straight sinus
- Inferior/superior sagittal
- Transverse
- Signmoid
- Cavernous
The cavernous sinus contains the internal carotid artery. It is the only place in the body where an artery runs through a venous supply. If the artery ruptures then it can cause an arteriovenus fistula.
Also passing through the cavernous sinus is the occulomotor, trochlear, opthalmic and maxillary nerves
Blood supply of the brain
|
Anterior/Carotid supply
|
Posterior/Basilar artery
|
n.b Central branches of MCA include lateral striate ateries. Blockage of these causes a classic stroke.
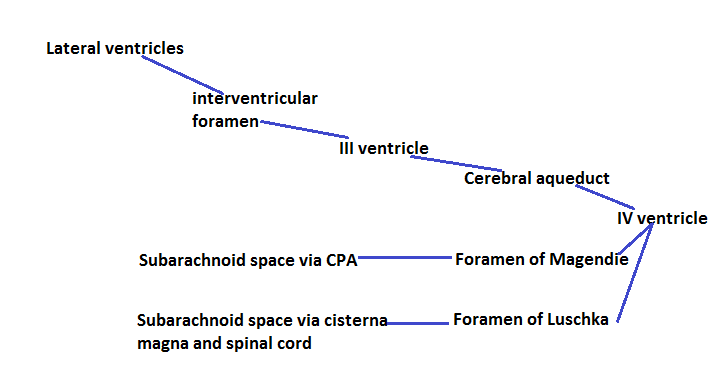
CSF pathway
Produced in choroid plexus (lateral venrticles)
Basal ganglia
Rostral (upper)
Striatum - putamen
- caudate nucleus
Globus pallidus - internal segment (GPi)
- external segment (GPe)
Caudal (lower)
Subthalamic nucleus
Substantia nigra
Caudate nucleus runs along wall of lateral ventricle
Putamen is lateral to caudate nucleus
Substantia nigra is in mesencephalon
Red nucleus is above substantia nigra
Subthalamic nucleus retrolateral to substantia nigra
There are several BG circuits
Striatum - putamen
- caudate nucleus
Globus pallidus - internal segment (GPi)
- external segment (GPe)
Caudal (lower)
Subthalamic nucleus
Substantia nigra
Caudate nucleus runs along wall of lateral ventricle
Putamen is lateral to caudate nucleus
Substantia nigra is in mesencephalon
Red nucleus is above substantia nigra
Subthalamic nucleus retrolateral to substantia nigra
There are several BG circuits
- motor
- limbic
- occulomotor
Illnesses associated with b.g dysfunction
Motor disorders
Psychiatric disorders
Secondary damage
n.b in PD there is not enough dopamine, in HD there is too much
Dopamine
- Parkinson's disease
- Huntington's disease
- Dystonia
- Gilles de la Tourette syndrome
Psychiatric disorders
- OCD
- ADHD
Secondary damage
- Cerebral palsy
- Wilson disease
n.b in PD there is not enough dopamine, in HD there is too much
Dopamine
- Tyrosine --> L-dopa --> Dopamine
- Dopamine switches off basal ganglia (allows movement)
- Stored in vesicles in substantia nigra
- Released across synapse via receptors in basal ganglia - nigrostriatal bundle (non functional in PD)
Basal ganglia disorders
Dystonia
Onset after adolescence
Occasionally precipitated by trauma
Sustained muscle contractions - twisting/repetitive movements/abnormal posture
Symptoms/signs
Primary - caused by pathology of CNS --> basal ganglia
Secondary - identified cause --> brain damage, post trauma/drugs, Wilson disease
Treatment
Gilles de la Tourette syndrome
Characterized by tics - motor and phonic
Causes
Pathophysiology
Diagnosis
Management
Parkinson's disease
Onset age 45-60.
Men>Women
Abnormally large protein aggregates develop in nerve cells in substantia nigra - Lewy bodies.
Neurons in substantia nigra synthesize dopamine - inhibits neurotransmission in corpus striatum
Degeneration - loss of dopamine in coprus striatum which correlates with degree of bradykinesia.
Symptoms/signs
Early motor symptoms - fine movements difficult
- stiff joints/limbs - ache
- slurred speech --> speech loss
Later onset cognitive - depression
- anxiety
Cause of death usually bronchopneumonia with immobility and cognitive impairment
>50% TH+ cell loss = symtomatic
Causes
Risk factors
Treatment
- can eventually cause L-dopa induced dyskinesia
Huntington's disease
Autosomal dominant (Hungtingtin gene)
35-45 y.o onset
Cerebral atrophy - marked loss of neurons in caudate nucleus/putamen
Reduced GABA in striatum - increased movement
Increased transglutamase in cortex, cerebellum and corpus striatum
Decreased GABA, ACE and met-enkephalin in substantia nigra
Increased somatostatin in corpus striatum
Dopamine levels normal
Symptoms/signs
early stage - subtle change in personality/cognition.physical skills
Diagnosis
Treatment
Death usually 10-20 years from onset
Onset after adolescence
Occasionally precipitated by trauma
Sustained muscle contractions - twisting/repetitive movements/abnormal posture
Symptoms/signs
- Continuous pain, cramping, relentless muscle spasms
- Abnormal posture
- Not obviously clumsy
- Patient may be able to relieve symptoms by touching affected area (geste antagonistique)
- Loss of precision muscle coordination (can't write, drop things etc)
Primary - caused by pathology of CNS --> basal ganglia
Secondary - identified cause --> brain damage, post trauma/drugs, Wilson disease
Treatment
- No cure
- Minimizing symptoms
- Neuro-suppression etc
Gilles de la Tourette syndrome
Characterized by tics - motor and phonic
Causes
- inherited - mode of inheritance unkown
- males>females
- psychosocial/environmental factors can influence severity
- Dystonias are a secondary cause
Pathophysiology
- Exact mechanism unknown
- Thought to result from dysfunction in the Basal Ganglia
Diagnosis
- Multiple motor and one or more phonic tics over the period of one year. No more than three consecutive tic free months.
Management
- Psychobehavioural therapy
- education
- neuroleptics (typical and atypical)
Parkinson's disease
Onset age 45-60.
Men>Women
Abnormally large protein aggregates develop in nerve cells in substantia nigra - Lewy bodies.
Neurons in substantia nigra synthesize dopamine - inhibits neurotransmission in corpus striatum
Degeneration - loss of dopamine in coprus striatum which correlates with degree of bradykinesia.
Symptoms/signs
- Tremor
- Bradykinesia
- Rigidity
Early motor symptoms - fine movements difficult
- stiff joints/limbs - ache
- slurred speech --> speech loss
Later onset cognitive - depression
- anxiety
Cause of death usually bronchopneumonia with immobility and cognitive impairment
>50% TH+ cell loss = symtomatic
Causes
- Idiopathic
- Drug induced - phenothiazines/butyrophenones
- Genetic mutations
Risk factors
- Age - mid to late years onset. Increased risk as age increases
- Gender - m>f
- Family history - genetic predisposition
- Oestrogen levels - post menopausal women/hysterectomy
- Environmental - herbicides/pesticides inhibit dopamine production
- Head trauma - damage to head/neck/cervical spine
- Genetic fractures
Treatment
- No cure
- Levodopa therapy - can cross BBB where it is converted to dopamine
- can eventually cause L-dopa induced dyskinesia
- Treat symptoms
- Physical therapy
- Palliative care
Huntington's disease
Autosomal dominant (Hungtingtin gene)
35-45 y.o onset
Cerebral atrophy - marked loss of neurons in caudate nucleus/putamen
Reduced GABA in striatum - increased movement
Increased transglutamase in cortex, cerebellum and corpus striatum
Decreased GABA, ACE and met-enkephalin in substantia nigra
Increased somatostatin in corpus striatum
Dopamine levels normal
Symptoms/signs
- Chorea - jerky, random, uncontrolled movements
early stage - subtle change in personality/cognition.physical skills
- rigidity
- writing motions
- abnormal posture
- physical inability
- abnormal facial expression
- difficulty chewing/swallowing/speaking
- cognitive planning, rule acquisition, telling what is acceptable socially
- depression
Diagnosis
- Generic testing
- Prenatal testing
Treatment
- Treatment
- Phenothiazines - sulpiride
- Tetrabenazine
- Treat symptoms
- Physical therapy
Death usually 10-20 years from onset
Cranial nerves
|
I Olfactory - sensory
II Optic - sensory III Occulomotor - motor IV Trochlear - motor V Trigeminal - both VI Abducens - motor |
VII Facial - both
VIII Vestibulocochlear - sensory IX Glossophayngeal - both X Vagus - both XI Accessory - motor XII Hypoglossal - motor |
Location
Above the pons (midbrain) - I, II, III, IV (olfactory and optic not in midbrain)
In the pons - V,VI,VII,VIII
In the medulla - IX, X, XI, XII
Above the pons (midbrain) - I, II, III, IV (olfactory and optic not in midbrain)
In the pons - V,VI,VII,VIII
In the medulla - IX, X, XI, XII
NerveOlfactory
Optic Occulomotor Trochlear Trigeminal -Opthalmic -Maxillary -Mandibular Abducens Facial Vestibulocochlear Glossopharyngeal Vagus Accessory Hypoglossal |
InnervationSensory
Sensory Motor Motor Both Motor Both Sensory Both Both Motor Motor |
PathwayPierces cribiform plate
Optic canal Superior orbital fissure Superior orbital fissure Superior orbital fissure Foramen Rotundum Foramen Ovale Superior orbital fissure Internal acoustic meatus Internal acoustic meatus Jugular foramen Jugular foramen Jugular foramen Hypoglossal canal |
FunctionOlfaction
Vision Eye movements Rotates eyeball Mastication Face sensation Jaw jerk Rotates eyeball Facial expression Balance/hearing Taste (post 1/3) Taste/speech /viscera Accessory muscles Tongue movement |
testSmelling salts
Fundoscopy Draw H Draw H Touch face Draw H Grit teeth Tuning fork Gag reflex Say aaahhh turn head/ shrug Stick out tongue |
Brainstem lesions
General somatic efferent column - basal plater, supplies trunk and limbs, occulomotor tochlear abducens and
tongue supply
General visceral efferent column - cranial parasympathetic system
General visceral afferent column - visceral territory of vagus and glossopharyngeal nerves
General somatic afferent column - receives from skin and mucous membranes (trigeminal)
Midline Structures
Motor pathway - contralateral arm/leg weakness
Medial lemniscus -contralateral arm/leg proprioception/vibration
Medial longitudinal fascicles - ipsilateral eye adduction failure
Motor nucleus and nerve - ipsilateral loss of CN III, IV, VI, XII function (divide into 12), other nerves in lateral
brainstem
Lateral Structures
Spinocerebellar pathway - ipsilateral arm/leg ataxia
Spinothalamic pathway - contralateral alteration of pain in limbs
Sensory nucleus - ipsilateral alteration of pain on face
Sympathetic pathway - ipsilateral homers syndrome
Therefore...
Medial brainstem lesion - 4 M's and relevant motor cranial nerves
Lateral (side) brainstem lesion - 4 S's and CN 9-11/5-8 lesion (pons/medulla)
n.b. if signs of both consider basilar artery occlusion/problem
Bells Palsy
Bulbar Palsy
III Nerve Palsy
VI Nerve Palsy
Guillan Barre
tongue supply
General visceral efferent column - cranial parasympathetic system
General visceral afferent column - visceral territory of vagus and glossopharyngeal nerves
General somatic afferent column - receives from skin and mucous membranes (trigeminal)
Midline Structures
Motor pathway - contralateral arm/leg weakness
Medial lemniscus -contralateral arm/leg proprioception/vibration
Medial longitudinal fascicles - ipsilateral eye adduction failure
Motor nucleus and nerve - ipsilateral loss of CN III, IV, VI, XII function (divide into 12), other nerves in lateral
brainstem
Lateral Structures
Spinocerebellar pathway - ipsilateral arm/leg ataxia
Spinothalamic pathway - contralateral alteration of pain in limbs
Sensory nucleus - ipsilateral alteration of pain on face
Sympathetic pathway - ipsilateral homers syndrome
Therefore...
Medial brainstem lesion - 4 M's and relevant motor cranial nerves
Lateral (side) brainstem lesion - 4 S's and CN 9-11/5-8 lesion (pons/medulla)
n.b. if signs of both consider basilar artery occlusion/problem
Bells Palsy
- Facial nerve palsy
- Ipsilateral loss of facial expression
- Failure to close eye
- Pain behind ear
- Absent corneal relfexes
- Certain sounds painfully loud (hyperacuisis)
Bulbar Palsy
- Cranial nerves that arise from medulla (IX, X, XI, XII)
- Dysphagia
- Slurring speech
- Dysphonia
- Excess saliva
- Wasting/fasciculating tongue
- No gag reflex
- Caused by MND/Guillan Barre syndrome
III Nerve Palsy
- Complete ptosis
- dilated/fixed pupil
- eye looks down/out
- Caused by PCA aneurysm, diabetes, uncal herniation (in temporal lobe)
VI Nerve Palsy
- Diplopia
- Horizontal gaze - eye can't look down midline
- Double vision
Guillan Barre
- Ascending paralysis - hands and feet, moving up toward trunk
- Weakness in lower limb
- Previous 'flu like' infection
- Low grade distal weakness
- Reduced reflexes
- Reduced sense/light/touch
- Upper limbs/CN normal
