Describe bony structure at both microscopic and macroscopic level:Major groups of bones in the skeleton:
Difference between cortical and trabecular bone:
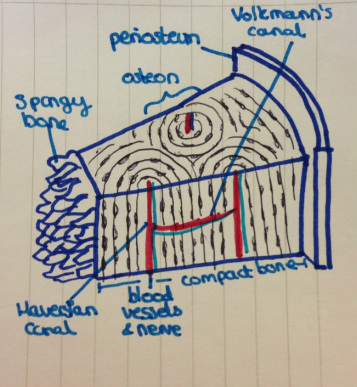
Bone is composed of:
Periosteum:
Endosteum:
|

|
describe bone metabolism:
- Bone is remodelled continuously once growth is complete, with the complete replacement of the axial skeleton happening every 7-10 years.
- Remodelling is the physiologically balanced process between resorption by osteoclasts (specialised macrophages) followed by reformation by osteoblasts which do so by secreting type 1 collagen (osteoid).
- And also differentiating into osteocytes whereby they deposit themselves as metabollically inactive cells amongst the deposited stroma.
- Osteoblasts and osteoclasts must be able to communicate.
- Coupling is where bone formation occurs at the sites of previous resorption.
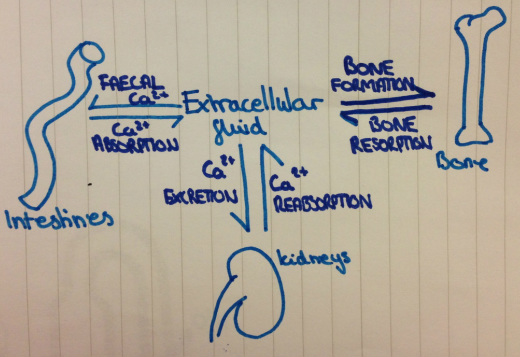
Calcium homeostasis:
Bone: Released rapidly from the exchangeable Ca on surface. Slowly by osteoclasts during bone reabsorption.
Kidney: Amount filtered through glomerulus depends on GFR and ultra-filterable calcium. 98% of filtered is reabsorbed (more if PTH increases, less if Na increases)
PTH:
- Increases Ca reabsorption
- Increases bone remodelling
- Increases bone resorption (>formation)
- Increases 1,alpha, hydroxlation of 21-OH vitamin D and therefore increases Ca absorption in gut.
Calcitonin:
- Produced by c cells in the thyroid. "Anti PTH"
- Stimulated by Ca increase
- Decreases bone resorption (decreases osteoclasts)
- Increases Ca excretion
Vitamin D:
- Increases Ca absorption in the gut
- Increases mineralisation in bone
- Increased Ca reabsorption.
describe the structure and function of spinal column/vertebra, cord and nerve roots:
- Vertebral column: Critical for locomotion, support of the upper trunk and head, stabilisation of the pelvis, posture and protection of the delicate structures of the spinal cord.
- 7 cervical vertebrae, 12 thoracic, 5 lumbar, 5 fused sacral vertebrae forming the sacrum, and 3-5 fused coccygeal vertebrae forming the coccyx.
- Each intervertebral disc composes the central, gelatinous nucleus pulposus and the outer annulus fibrosis. Above and below each disc is a cartilage plate centrally, and an outer epiphyseal ring, which the annuli insert into.
- Grey matter composed of interneurons, the cell bodies and dendrites of efferent neurones, the entering axons of afferent neurones, and glial cells.
- The regions of grey matter projecting towards the back of the body are called dorsal horns, whereas those oriented toward the front are the ventral horns.
- The grey matter is surrounded by white matter, which consists of groups of myelinated axons. These groups of fibre tracts run longitudinally through the cord, some descending to relay information from the brain to the spinal cord, others ascending to transmit information to the brain. Pathways also transmit information between different levels of the spinal cord.
- Groups of afferent fibres that enter the spinal cord from the peripheral nerves enter on the dorsal side of the cord via the dorsal roots.
- Small bumps on the dorsal roots, the dorsal root ganglia, contain the cell bodies of these afferent neurones.
- The axons of efferent neurones leave the spinal cord on the ventral side via the ventral roots.
describe features of a focussed history on back pain:
- How the pain started? Sudden or gradual?
- Pattern, intensity and duration of current episode.
- Exacerbating/relieving factors
- Related symptoms- leg pain, weakness or numbness, problems with bowels or bladder.
- Spine problems
- Arthritis
- Previous episodes and treatment
- Previous accidents or injuries
- FHx
- Work history
- Exercise/sporting activities
- History of cancer or other illnesses.
- Recent fever or unexplained weight loss.
- Corticosteroid use
- Smoking history
describe the 'red flag' symptoms in a back pain history:
|
Damage to S2,3,4: (S2,3,4 keeps poo and wee of the floor)
|
list the causes of back pain in a logical and systematic manner:
Mechanical
Neoplastic
- Intervertebral disc degeneration
- Wearing down of the facet joints
- Muscle tension
- Spasms
- Ruptured discs/herniated discs
- Sprains (tears in the ligaments that support the spine- twisting of not lifting properly)
- Fractured vertebrae- can be a results of osteoporosis.
- Scoliosis- presents with curvature of the spine in middle age.
- Spondyloarthropathy (Night time waking with pain and stiffness, morning stiffness in the back, low back pain that improves with activity, age <40)
- Arthritis- OA, RA, ankylosing spondyloarthritis
- Spinal stenosis
- Cauda equina syndrome
Neoplastic
- Primary
- Metastatic
- Vertebral osteomyelitis
- Epidural abscess
- Septic discitis
- Osteoporotic compression fractures
- Paget’s disease
Risk factors for osteoporosis:
Risk factors for osteoporosis
Fixed risks for osteoporosis include:
Age, Female gender, Family history, Previous fracture, Race/ethnicity, Menopause/hysterectomy
Long term glucocorticoid therapy, Rheumatoid arthritis.
Secondary risk factors
Medical treatments affecting bone health
Fixed risks for osteoporosis include:
Age, Female gender, Family history, Previous fracture, Race/ethnicity, Menopause/hysterectomy
Long term glucocorticoid therapy, Rheumatoid arthritis.
Secondary risk factors
- Asthma
- GI problems (Crohn’s disease etc.)
- Rheumatoid arthritis
- Haematological disorders/malignancy
- Some inherited disorders
- Hypogonadal states (Turner syndrome/Kleinfelter syndrome, amenorrhea etc.)
- Endocrine disorders (Cushing’s syndrome, hyperparathyroidism, diabetes, etc.)
- Immobility
Medical treatments affecting bone health
- Glucocorticoids
- Certain immunosuppressant (calmodulin/calcineurine phosphatase inhibitors)
- Thyroid hormone treatment
- Aromatase inhibitors
- Certain antipsychotics
- Certain anticonvulsants
- Certain antiepileptic drugs
- Lithium
- Methotrexate
- Antacids
- Proton pump inhibitors
